In our Bacterial World exhibition we offer a selection of ten bacteria that have changed the world, some in profound ways. In this series of short fact-file posts we present one of the ten each week. This week’s bacteria are…
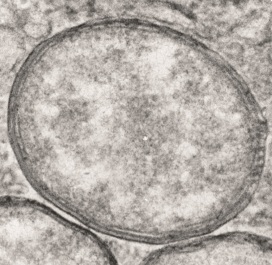
Wolbachia
– the man-killers
Where they live Up to 60 percent of insect species are infected with the bacterium Wolbachia, as are other species such as nematode worms.
Why they are important Wolbachia selectively kills off males in many species of insect and alters the sex ratio of the population to its own advantage. However, some species of insect rely on it for protection against other threats.
How they are named
The bacteria take their name from Simeon Burt Wolbach, who along with Marshall Hertig co-discovered Wolbachia in 1924 in a mosquito.
How they work Infected female insects pass the Wolbachia to their offspring – so the bacteria do everything they can to ensure females survive. Their strategies include killing male larvae, making males infertile, and rendering females able to reproduce without males.
Top image copyright: Joshua Blight (University of Oxford) & Steven Sinkins (University of Glasgow)
In our Bacterial World exhibition we offer a selection of ten bacteria that have changed the world, some in profound ways. In this series of short fact-file posts we present one of the ten each week. This week’s bacteria are…
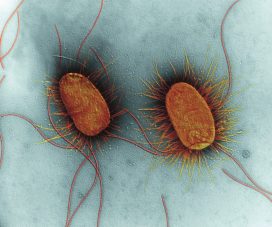
Escherichia coli
– the medicine-manufacturers
Where they live Millions of Escherichia coli live harmlessly in your gut, keeping more dangerous bacteria at bay. A few strains cause food poisoning.
Why they are important E. coli can act as a protein factory, accepting genes from other species and reproducing them. By combining DNA from more than one source, scientists can manipulate E. coli so that it manufactures human insulin.
How they are named Escherichia coli’s name reflects its discoverer, Theodor Escherich, and the fact that he found it in the human colon.
How they work Bacteria often contain plasmids, extra DNA rings that confer particular properties. Researchers can introduce genes into E. coli using plasmids, enabling the bacteria to make all kinds of biotechnology products from foods to medicines.
Top image: Coloured transmission electron micrograph (TEM) of two Escherichia coli bacteria. E. coli are Gram-negative bacilli (rod-shaped) bacteria. Long flagellae (thin thread-like structures) are used by the bacteria to move themselves. The spiky filaments on the sides of the bacteria are pili, thin strands of protein used when two bacteria conjugate (transfer DNA). E. coli is a normal inhabitant of the human intestine. However, under certain conditions its numbers may increase, causing infection. Magnification: x17,200 at 10 centimetres high. Copyright: Science Photo Library
In our Bacterial World Science Short event series, researchers present their latest findings related to themes in the exhibition. At a recent Science Short, Hannah Behrens, a University of Oxford PhD student, explained how bacteria become resistant to antibiotics and how the species-specific antibiotics she studies might reduce the worrying rise in antimicrobial resistance.
Bacteria that are resistant to antibiotics present a huge problem. I work on developing new antibiotics that will slow the development of bacterial resistance.
But let’s not get ahead of ourselves. Your body is full of bacteria. In fact, there are more bacteria than human cells in your body. Most of these bacteria are good for you; they help you digest food and protect you from diseases.
But once in a while a harmful bacterium causes an infection. This could be a lung, wound, or bladder infection, or something with a fancy name like, Black Death, tuberculosis, leprosy, syphilis or chlamydia. The doctor will then prescribe you antibiotics to kill the offending bacteria.
Hannah Behrens delivers her Science Short talk at the Museum
The development of antibiotics in the 20th century was a major breakthrough. For the first time bacterial infections could be effectively and rapidly treated. Since 1942, when antibiotics first became available, we have discovered many new antibiotics which have saved millions of lives.
However, in the last 30 years we have not managed to develop any new antibiotics. During the same time, many bacteria have adapted to become resistant to the antibiotics we do have. In 2017, a woman in the US died because she had an infection with bacteria that were resistant to all available antibiotics. It is estimated that already 700,000 people in Europe alone die because of resistant bacteria per year. What is happening?
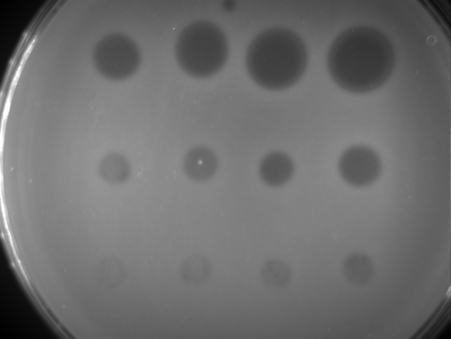
Bacteria are forming a lawn on this plate (light areas); where an antibiotic has been spotted on the bacteria they die and leave the surface blank (dark areas).
Every time we treat bacteria with antibiotics, most die, yet a few resistant bacterial cells survive. Like Rudolph the red nosed reindeer, the resistant bacteria are usually at a disadvantage until a special situation arises (a foggy night for Rudolph; treatment with antibiotics for resistant bacteria).
Under usual circumstances, producing a resistance mechanism is a disadvantage: it wastes energy and slows down growth, so very few bacteria are resistant. Only when all the non-resistant bacteria are killed by antibiotics do the resistant ones thrive. They have no more competition, and have all the resources, such as food and space, to themselves.
The more we use antibiotics, the more resistant bacteria we get. It is essential not to use antibiotics carelessly.
More antibiotics are used in animal farming than on humans. If we eat less meat, and so reduce the farming of livestock for food, we may reduce the growth of resistance bacteria. Another approach is to only take antibiotics when the doctor prescribes them. Antibiotics do not help against viral infections like colds. In many low and middle income countries, antibiotics are available in supermarkets and it is no coincidence that these countries have higher levels of resistant bacteria.
The precision antibiotics research group in the Department of Biochemistry at the University of Oxford
Apart from avoiding the unnecessary use of antibiotics, scientists – including me – are trying to develop better therapies against bacteria. I study precision antibiotics: drugs that specifically kill one species of bacteria. The advantage of this is that all good bacteria remain unharmed and only the disease-causing species is targeted. This also means that only resistant bacteria from this one species get an advantage to thrive.
I am interested in species-specific antibiotics against Pseudomonas aeruginosa. This bacterial species causes lung and wound infections and, according to the World Health Organization, is one of the three bacteria for which we most urgently need new antibiotics. Colleagues of mine tested different precision antibiotics against Pseudomonas and found one that is better than the others, called Pyocin S5.
Hannah’s painting of how researchers think pyocin antibiotics kill bacteria. The pink bacterium produces pyocins (pink balls), which enter the susceptible blue bacteria through pores (blue). The blue bacteria mistake the antibiotic for a nutrient and open the pore to let it in. Once inside the bacterium it forms a pore in the inner membrane which causes leakage of the cell contents and kills the cell.
I am now investigating how stable this antibiotic is, how it recognises this specific species of bacteria and how it enters the bacterial cells. This knowledge is important to decide on how to store, transport and administer the drug. I also hope that understanding why Pyocin S5 is more effective than the other antibiotics will allow us to design more effective, targeted antibiotics in the future.
My hope is that one day we will treat all bacterial infections with precision antibiotics and that antibiotic resistance will become a problem of the past.
Once found in almost every museum and university in the western world, human anatomy collections have slowly disappeared over time, as medical practices have changed. These collections are historically important and medically relevant, providing direct evidence of patients’ lives and illustrating a pivotal period in the history of medicine.
Over the past seven months, Dr Kathryn Krakowka has been going through the Museum’s human remains specimens to create a new detailed database of the contents. Here, Kathryn talks about the fascinating material she is working on…
The Museum holds many specimens that are not on public display, and perhaps one of the largest collections hidden from view is the human remains. This collection was started in the first half of the 18th century by Dr Matthew Lee, and eventually passed to Dr Henry Acland, founder of the Museum. Acland added a lot to the collection, acquiring his own samples as well as purchasing specimens and collections from other physicians.
When Acland gathered material for the new museum building in 1860, he brought this anatomical and physiological material with him, including the human remains. The collection continued to develop throughout the 19th century and grew to contain over 1,400 specimens. It is now one of the few collections from this period still in existence in Britain.
As a specialist in human osteology, I am trained to assess human skeletonised remains for such characteristics as sex, age-at-death, and any pathologies or trauma that the individual was affected by in life.
The Museum’s collection revealed specimens that tell a tale of health and medicine at Oxford in the 18th and 19th centuries. Many of the specimens were used to teach medicine, so many different skeletal pathologies are represented, including bacterial infections, genetic deformities, nutritional deficiencies, and traumatic injuries.
A skull fragment showing a large growth. The four round marks are thought to have been made by a tool during investigations after death.
One example is the frontal bone of a possible child, pictured above. This presents a large porous growth affecting both the outer and inner table of the bone. The characteristics of the lesion suggest osteosarcoma (bone cancer). There are then what appear to be four tool markings on the outer table of bone that indicate some sort of drill may have been used to take samples of the bone after death, possibly in an attempt to determine what was ailing the individual during life.
As this growth is quite large and just above the forehead, it would have been very noticeable while the individual was alive. This specimen provides an interesting example of how medical practices were often developed through exploratory postmortem analysis.
Now that the collection has been fully catalogued and digitised, it is hoped that further research into specimens like this one can help shed light on historical pathologies and the development of medicine as a discipline.
The database and digital images of the specimens will soon be available on the Museum’s website, thanks to funding by the John Fell Fund.